Retake
P16) Arm pain and lethargy in an infant
Review the Learning Outcomes, Hx, PE and Labs, and begin the module with your Provisional Diagnosis. Keep hitting "Next" to move through the module.
Learning Outcomes
- Articulate your relationship with the consulting diagnostic radiologists in the evaluation of a pediatric patient with pain after a fall.
- Review the DDx considerations in a pediatric patient with pain after a fall.
- Identify the spectrum of imaging findings in appropriate modalities for evaluating a pediatric patient with pain after a fall.
History
A 6-week-old male infant is brought to the emergency department by his mother. She reports that the infant has been excessively fussy and irritable over the past couple of days, with right arm pain and decreased feeding and lethargy. The mother denies any known trauma or falls but is concerned due to the infant's worsening symptoms. She provides a vague history, stating that she is unsure how the injuries occurred. The mother mentions that the infant's older sibling, a 3-year-old, has been around the baby but denies any aggressive behavior. Upon further questioning, the mother's account of events changes slightly, and she mentions that the infant may have fallen off the couch onto a carpeted floor.
Physical Exam
BP: 100/56, HR 160, RR 45, Temp 98F, O2 saturation 98%.
• General: The infant appears to be in distress, irritable, and difficult to console.
• HEENT: Head is normocephalic. Pupils are equal, round, and reactive to light.
• Neck: Supple with no palpable masses or lymphadenopathy.
• Chest: Bilateral chest wall tenderness palpation. Breath sounds are clear and equal bilaterally.
• Cardiac: Tachycardic with a regular rhythm. No murmurs, gallops, or rubs.
• Abdomen: Soft, non-distended, and non-tender. Bowel sounds are present.
• Extremities: Severe tenderness to palpation and deformity of the right proximal arm. Right and left distal forearms are tender to palpation.
• Neurologic: Moving all extremities but with pain. Moro reflex present.
Labs
None
Provisional Diagnosis
Select the Dx you believe is most appropriate
This 6-week-old male infant presents with multiple injuries, including swelling over the right parietal region, chest wall tenderness, and severe tenderness with deformity in the right proximal arm. The mother provides an inconsistent history, mentioning a possible fall from a couch, but the severity and extent of the injuries are not consistent with this explanation. Given the infant's age and the presence of multiple severe injuries, there is a high suspicion for non-accidental trauma.
Well done. You were correct
Potential Acuity
What is your assessment of the likely acuity for this patient?
Well done. You were correct
This patient requires urgent workup and management.
First Imaging Study
What is the first imaging study you will order?
A skeletal survey is the appropriate imaging modality for suspected non-accidental trauma in young children, as it detects occult fractures, identifies specific fracture patterns suggestive of abuse, and evaluates healing fractures indicating a history of repeated trauma.
Well done. You were correct
Pertinent Imaging Observations
Click on the links below to view images from the study, and assess these key findings as best you can.
Skeletal survey
Which bone(s) in the right arm have fractures?
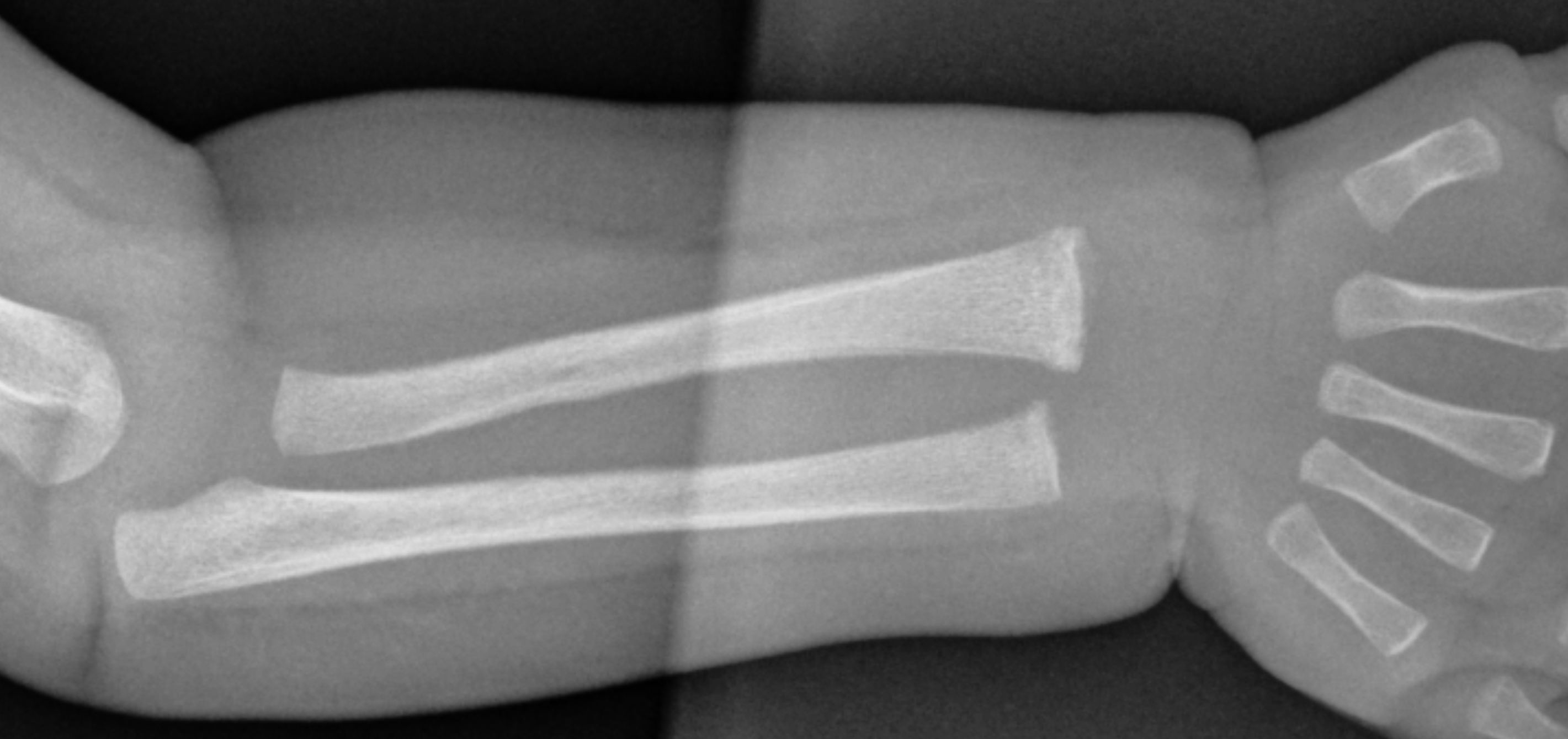
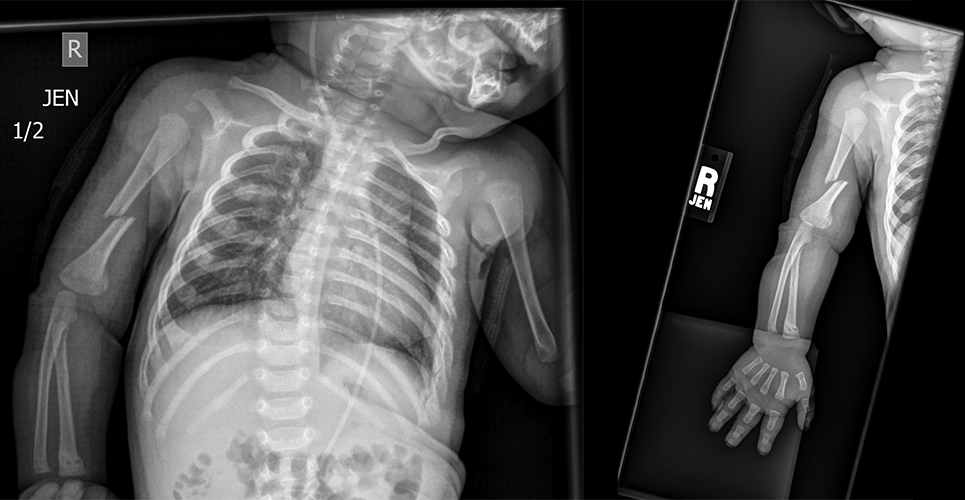
The right mid-humeral shaft has an acute fracture, while the right distal humerus, radius, and ulna have healing fractures.
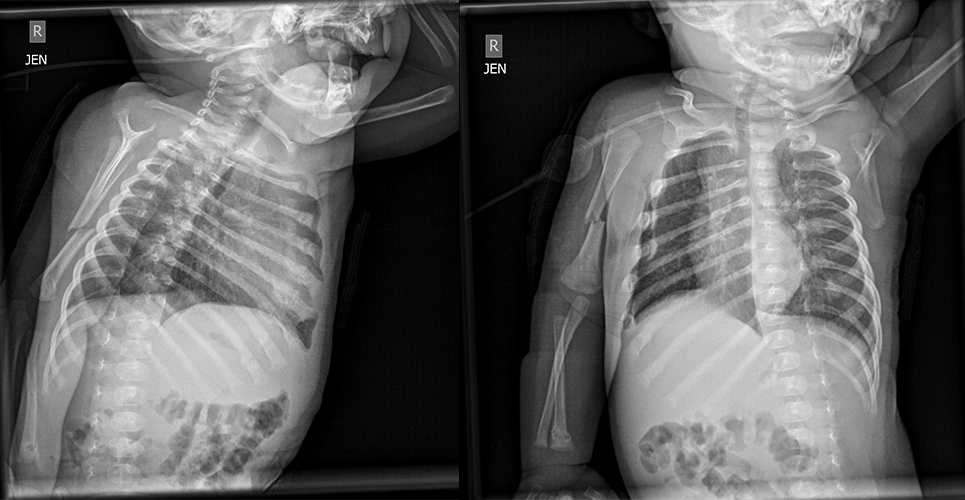
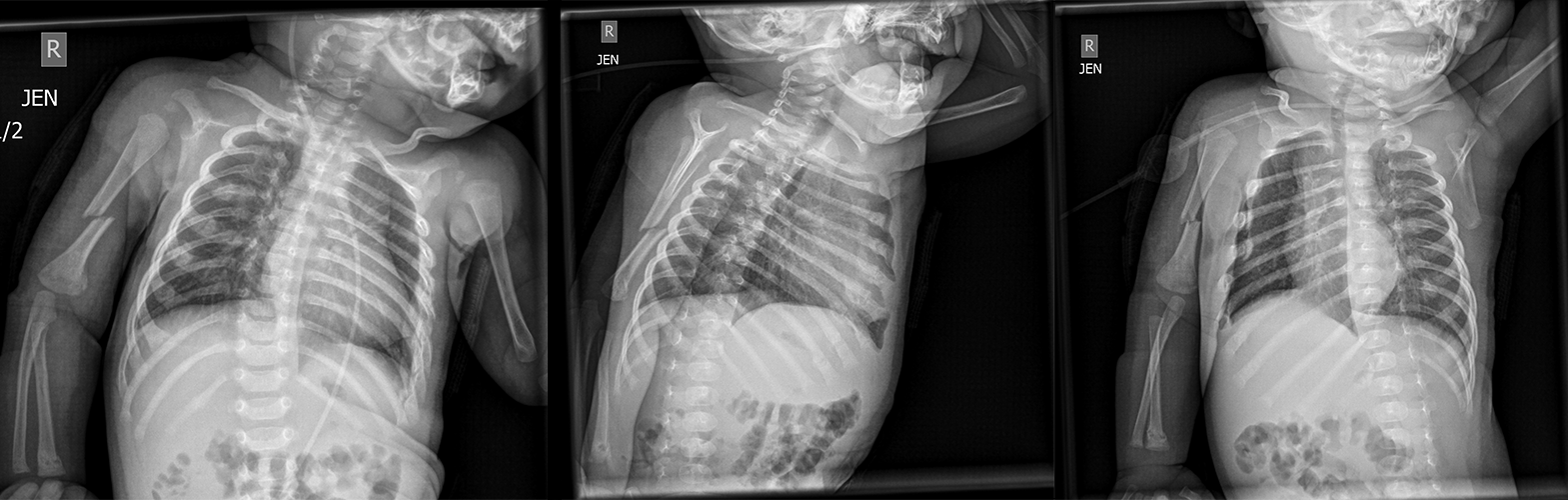
In the ribs, there are:
There are healing fractures in several bilateral ribs.
The fractures appear:
The fractures are of different ages, as some are acute (e.g., right mid-humeral shaft) and others are healing (e.g., right distal humerus, radius, ulna, and ribs).
In the left radius, there is:
There is a left radial metaphyseal corner fracture, which is a type of injury commonly associated with non-accidental trauma in young children.
View the full study if you'd like to take a look yourself.
Second Imaging Study
What is the next imaging study you will order?
Given the absence of intracranial injury indicators (neurological changes or facial injuries), a CT head might not be necessary. Likewise, a body CT may not be required as there are no signs of visceral injury besides the healing rib fractures. Bone scintigraphy is typically used as a supplementary exam to detect hidden, equivocal, or subtle injuries on plain radiographs.
Well done. You were correct
What is your Diagnosis now that you have seen the imaging results?
The patient’s presentation and imaging findings are consistent with non-accidental trauma.
Current Acuity
Initially, you selected and we suggested acuity.
Has your concern for this patient changed?
The patient requires urgent workup and management.
Assessment and Plan
Please provide your assessment and plan for this patient
The 6-week-old male infant presents with multiple healing rib fractures, an acute fracture of the right mid humerus, a metaphyseal corner fracture of the left distal radius, and healing fractures in the right distal humerus, right distal radius, and right distal ulna. The inconsistent history provided by the mother and the severity of the injuries raise a high suspicion for non-accidental trauma. The infant should be admitted to the hospital for close monitoring and further management, with consultations from pediatric orthopedic surgery for fracture management, and appropriate analgesia for pain management. Social work and child protective services should be involved to investigate the possibility of abuse and ensure the safety of the patient. Ongoing support and resources should be provided to the family.
Lessons Learned:
- Promptly identifying potential child abuse is crucial for treating the existing condition and safeguarding the child from future, potentially more serious harm. Abused children face up to a 50% risk of experiencing further abuse and a 10% risk of death if the abuse goes undetected at the initial presentation.
- Several historical factors can raise suspicion for abuse, such as inconsistent or vague accounts, implausible stories, or histories that change among different caregivers. Physical findings that may indicate abuse include injuries that don't align with the given history, injuries with patterns suggesting a method of infliction, and multiple injuries at various stages of healing.
- Fractures that are highly specific to non-accidental injuries include metaphyseal fractures, rib fractures, particular skull fractures, scapular fractures, sternal fractures, and outer third clavicular fractures. Other fractures that may be seen in non-accidental trauma include bilateral fractures with fractures of varying ages, digital fractures in non-ambulatory children, vertebral fractures, spiral humeral fractures, and epiphysis separation, middle clavicular fractures, linear simple fractures of the parietal bone, single diaphysis fractures, and greenstick fractures.
- The primary imaging modality for suspected non-accidental trauma is a skeletal survey,
- After assessing and addressing the child's urgent medical needs, the clinician should evaluate the suspicion level for child abuse, preferably in consultation with a multidisciplinary child abuse team. Reporting to the appropriate governmental authorities is often mandatory for suspected abuse cases, and hospitalization might be necessary for treating specific conditions or ensuring the child's safety.
Socioeconomic Factors: Factors that may contribute to a higher likelihood of non-accidental trauma include diminished self-esteem, depression, previous suicide attempts, significant life stressors, history of foster care or abandonment in childhood, unintended or unwanted pregnancies, and a past marked by relationship issues with other adults.
That's the end of the module! Once you've reviewed the video(s), you can click here for another case challenge.
Next


{kind=link}
{kind=link}
{kind=link}
{kind=link}